|
Click here or on the image below to read A Tribute to Prof.  Professor W. R. Proffit 1936-2018 You can also find A Tribute to Prof on the Think Piece Page, by clicking the link in the navigation bar above.
3 Comments
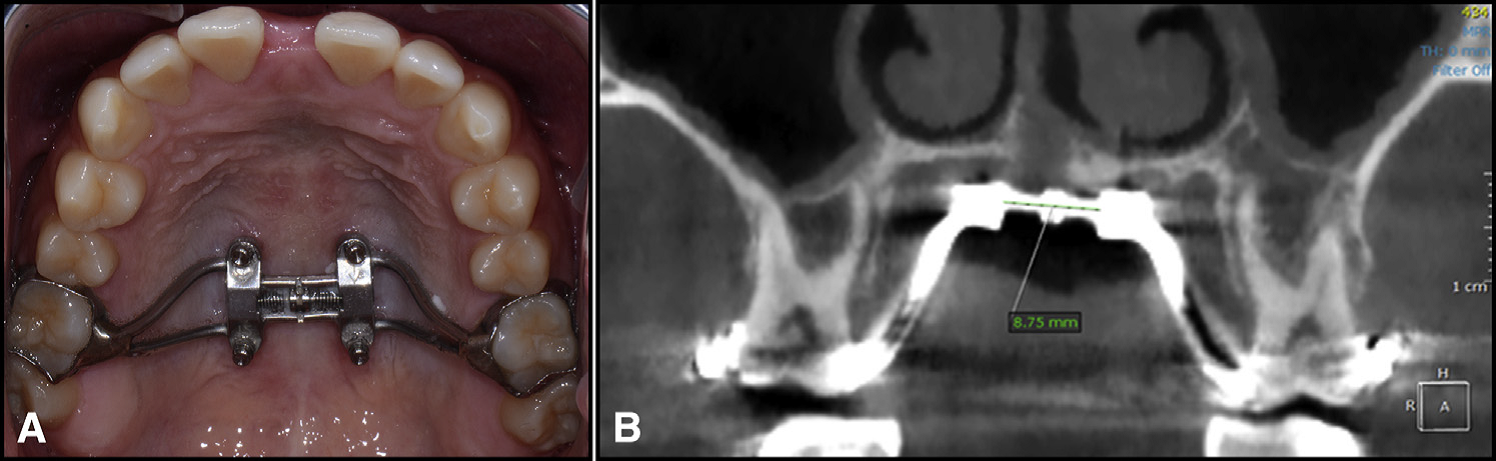 A modified Wilmes-style expander was used in all patients – with 4 mini-implants in the palate, and attachment to the first molars. (from Cantarella et al.) A modified Wilmes-style expander was used in all patients – with 4 mini-implants in the palate, and attachment to the first molars. (from Cantarella et al.) BY TATE H JACKSON AND TUNG T NGUYEN STUDY SYNOPSIS A group at the University of California at Los Angeles (UCLA) have conducted a retrospective study to evaluate how rapid palatal expansion with mini-implants placed in the palate works in post-pubertal patients. 15 participants (9 female) with ages ranging from 13.9 to 26.2 years were all consecutively-treated with a modified Wilmes-style hybrid tooth-borne / mini-implant borne maxillary expansion appliance. 14 of these patients were in dental crossbite. The need for expansion was determined by measuring and comparing maxillary and mandibular casts, not by comparison to population norms. All participants were treated with the hybrid tooth/mini-implant expander alone; no other appliances were in place during expansion. The authors report that all mini-implants were placed in the posterior palate with bicortical anchorage. The hybrid expander was turned twice each day (0.25mm per turn) until “a diastema appeared” and then just once per day. The expansion devices were maintained for 3 months following the end of activation. Cone-beam CT (CBCT) images were obtained for each participant before treatment and within 3 weeks of the end of active expansion, but before any additional active appliances were placed. After cranial base superimposition of the pre- and post-expansion volumes, transverse expansion was measured in coronal sections at the level of the Upper Zygoma (frontozygomatic suture), Lower Zygoma (zygomaticomaxillary suture), and Maxillary Molars. Expansion resulted in little transverse change at the Upper Zygoma [mean of 0.52mm (SD 0.37mm]. An average of 4.62mm (SD 1.33mm) of expansion occurred at the Lower Zygoma, and 8.33mm (SD 2.29mm) occurred at the Molar. Taken together, for every 1mm of transverse expansion, the zygomaticomaxillary complex rotated outward by 0.6 degrees on each side. Stated another way, an average of 6.8mm in expansion at the level of the jackscrew resulted in an average of 8.33mm of expansion at the molars, with an average of 2 degrees of total outward tipping of the molars on each side. It is important to note that tipping of the molars was highly variable, with standard deviations reported that were nearly double the mean. 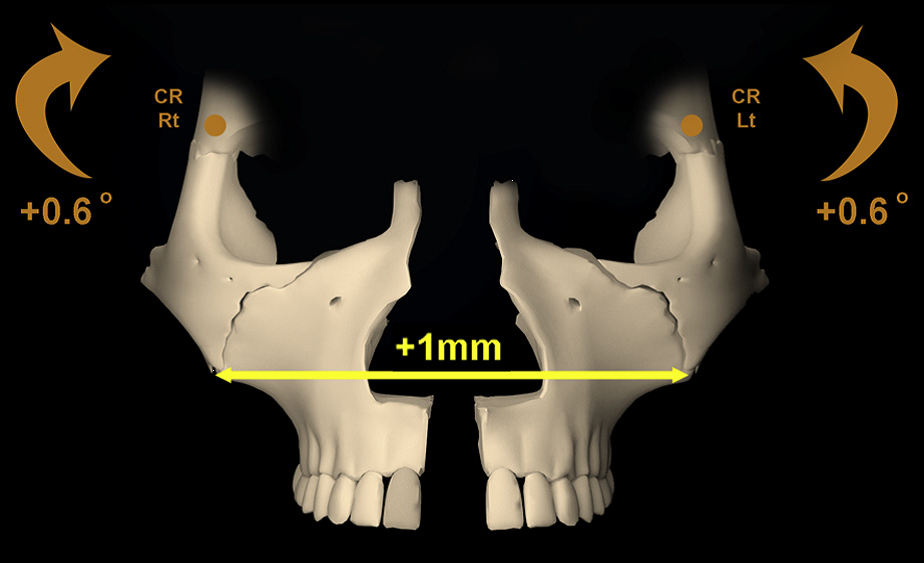 For every 1mm of total expansion at the midline, each half of the zygomaticomaxillary complex rotated outward by 0.6 degrees. (from Cantarella et al.) For every 1mm of total expansion at the midline, each half of the zygomaticomaxillary complex rotated outward by 0.6 degrees. (from Cantarella et al.) WHAT THE PROFESSORS THINK
The consecutive case series reported in this paper represents a well-constructed study, despite the limitations of retrospective data analysis. Superimposition of CBCT volumes and analyses of transverse changes were founded on validated methods, and reliability of the measurement made were adequately measured and reported. It is unfortunate that the authors did not report the rate of adverse outcomes for the participants in the study. e.g. Did any of the mini-implants fail? The paper focused a bit more on theoretical biomechanical outcomes, such as where the center of rotation might be for the skeletal units involved, than is likely to be helpful for practicing orthodontists. Some practical points can be gleaned, however: 1. When using a hybrid bone/tooth borne maxillary expander in later-adolescent to early adult patients, you should expect some “tipping” of the molars. That tipping happens due to a combination of skeletal rotation, and to a lesser degree, change in inclination of the molars. 2. Based on this study alone, the amount of molar tipping that occurs can be quite variable. As little as 4 degrees of total tipping might occur, or as much as 10 degrees. From previously published studies, the amount of tipping using mini-implants should certainly be expected to be less than with tooth-borne expansion alone, however. (1, 2) 3. In order to give a patient good estimates of the likelihood of both success and adverse outcomes with this treatment, more data are needed. These data represent good initial guide-points for orthodontists in practice and suggest that mini-implant maxillary expansion should be considered in younger non-growing patients with skeletal transverse issues. The prudent orthodontist, however, will communicate with the patient / parents that although the procedure is a great alternative to more invasive surgery, it still carries with it some real risk and uncertainty at this time. Article Reviewed: Cantarell D, et al. Midfacial changes in the coronal plane induced by microimplant-supported skeletal expander, studied with cone-beam computed tomography images. Am J Orthod Dentofac Orthop 2018; 154:337-345 (Sept). References: 1) Lin L, Ahn HW, Kim SJ, Moon SC, Kim SH, Nelson G. Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod. 2015;85:253–262 2) Mosleh MI, Kaddah MA, Abd ElSayed FA, ElSayed HS. Comparison of transverse changes during maxillary expansion with 4-point bone-borne and tooth-borne maxillary expanders. Am J Orthod Dentofacial Orthop. 2015;148:599–607.  Click the image below to read Dr. Proffit and Dr. Ackerman's review of the sensationalist book, Jaws.
You can also find the review on the Think Piece Page in the navigation bar above. 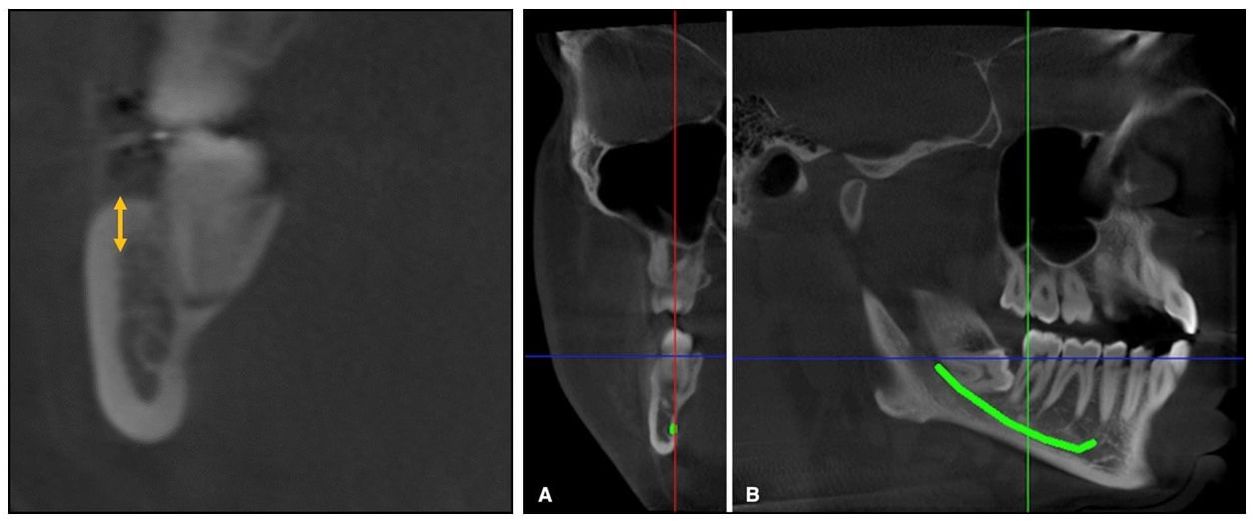 From Elshebiny et al. Coronal slice at the distal of the second molar (left), and the traced inferior alveolar canal (A and B). From Elshebiny et al. Coronal slice at the distal of the second molar (left), and the traced inferior alveolar canal (A and B). By WILLIAM R. PROFFIT, DDS, PhD STUDY SYNOPSIS At the Case-Western Reserve Dept. of Orthodontics, cone-beam CT images were used to evaluate the shape and location of the mandibular buccal shelf below the molars in white (European descent) patients as possible sites for skeletal anchorage. The cortical bone at this location has been used by orthodontists working with Asian patients, and excellent success (93%) with bone screws there has been presented.(1) The objectives in this study were to:
Cone-beam CT images for 30 adolescent white patients who had CBCT’s as part of their diagnostic evaluation were used to obtain a detailed view of the mandible in the first and second molar region (Figures 1 and 2). Cortical shelf thickness and the width of the buccal shelf bone were measured at the distal of the first molar and at the mesial and distal of the second molar. Then, the position of the mandibular nerve at these locations was established and its distance from a visual screw placed vertically was measured. The data showed that cortical bone thickness was greatest below the disto-buccal cusp of the second molar (8.1 + 1.3 mm), and that although this also was the point of greatest proximity to the mandibular neurovascular bundle (5.5 + 1.6 mm), this amount of clearance would provide adequate safety. Based on these measures, the authors recommended a 10 mm anchorage screw with a 5 mm screw head extension in this location. Locations below the first molar, not the second molar, have been recommended for Asian patients. Whether this recommendation is related to a clinically significant difference in mandibular anatomy between the two racial groups is not known. WHAT THE PROFESSOR THINKS
Alveolar bone screws have proved to be acceptable as anchorage for minor tooth movement but disappointing as anchorage for major tooth movement. For example, two clinical trials of a Nance lingual arch vs. alveolar bone screws for maxillary incisor retraction found no advantage with the bone screws—the two anchorage types were equally ineffective. It has become clear that cortical bone of the palate does offer almost perfect anchorage for intrusion, retraction and protraction of maxillary dental segments or the whole maxillary dental arch(2), and palatal anchorage now is preferred. Is the cortical bone of the buccal shelf of the mandible equally superior to mandibular alveolar bone? The existing data from Asian patients certainly indicates that for them, it is. This report for white adolescents shows that:
Based on these points, it is reasonable to expect bone anchors in the buccal shelf to be more stable than bone screws in the mandibular alveolus. However, there are no studies yet with high-quality outcome data for white patients to be certain that this is correct. Should American clinicians now start using bone screws into the mandibular buccal shelf for white as well as Asian patients when movement of mandibular segments or the whole mandibular arch is needed? On balance, I would say yes. Article Reviewed: Elshebiny T, Palomo JM, Baumgartel S. Anatomic assessment of the mandibular buccal shelf for miniscrew insertion in white patients. Am J Orthod Dentofac Orthop 2018; 153:505-511 (Apr). References
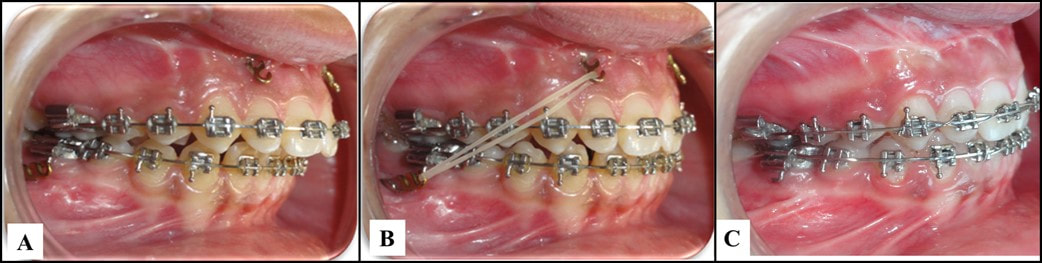 A, The miniplates after the healing period; B, application of the intermaxillary elastic; C, finishing to Class I molar and canine relationships. From Al-Dumini et al. 2018. A, The miniplates after the healing period; B, application of the intermaxillary elastic; C, finishing to Class I molar and canine relationships. From Al-Dumini et al. 2018. By TATE H. JACKSON and TUNG T. NGUYEN STUDY SYNOPSIS The use of skeletal anchorage for true orthopedic effect in growing Class III patients has now been well documented. Might the same strategy, using skeletal plates in both the maxilla and mandible, be effective to modify mandibular growth in Class II patients? A recent publication provides some initial evidence that it might. 28 growing children (age 11.83 +/- 0.83 years) with an ANB of 5 or greater, an OJ of 5mm or greater, and a ½ cusp Class II buccal relationship or greater were all treated with a standardized protocol by a single orthodontist. Each patient first went through alignment with fixed appliances for an average of 7 months before miniplates were placed in the anterior maxilla (2 just distal to the lateral incisors) and posterior mandible (2 just distal to the first molar). A cephalometric radiograph was taken after alignment and just before orthopedic traction began. Patients were instructed to wear intermaxillary elastics to the bone plates full-time beginning 20 days after plate fixation. The plates were ultimately loaded with ~450g on each side, and orthopedic traction was carried out for an average of 9 months. Another cephalometric radiograph was taken once each patient had a Class I molar and canine relationship and 1-3mm of OJ. Cephalometric superimposition of the pre-orthopedic and post-orthopedic radiographs were compared to non-treated Class II controls from another recent study matched based on age, race, observational period, gender, and skeletal maturity. Compared to controls, patients with Class II bone plates showed a significant:
WHAT THE PROFESSORS THINK
This study represents a nice initial approach to a topic for which randomized controlled data might be very difficult to obtain. The use of cephalometric radiographs following alignment and then immediately after orthopedic traction was a clever way to help account for potentially confounding tooth movement as a part of Class II correction. Using a well-matched control group of untreated Class II patients from a cohort who were apparently followed recently strengthens the data – despite the fact that 2D cephalometric analysis has limitations. It is key to note that the orthopedic effects reported (most importantly, mandibular elongation/forward-positioning) are not only larger than those described in meta-analyses with the use of more traditional appliances such as a Herbst or Twin-Block, but also that the 95%CI range is small (3.15-4.51). Of further clinical importance are the rotational mandibular changes and the overall combination of ANB and OJ reduction, with an accompanying increase in OB and uprighting of the incisors. Together, these changes suggest an absence of the dentoalveolar side-effects seen with functional appliances. What’s the bottom line for clinicians? Bone anchors, not surprisingly, show great promise for true orthopedic correction of Class II skeletal relationships, through a combination of elongation/forward-positioning of the mandible, as well as maxillary restraint. The use of skeletal plates for growth modification in Class II patients should be considered when:
Article Reviewed: Al-Dumanini et. al. A novel approach for treatment of skeletal Class II malocclusion: Miniplates-based skeletal anchorage. Am J Orthod Dentofac Orthop 153:239-47. 2018 |
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed