 Manuel Nienkemper et al. The Angle Orthodontist September 2015 Manuel Nienkemper et al. The Angle Orthodontist September 2015 BY WILLIAM R. PROFFIT
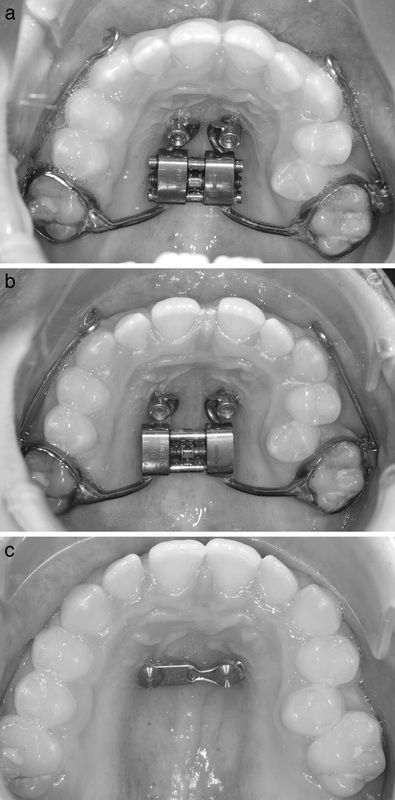
STUDY SYNOPSIS A recent study published in the Angle Orthodontist from authors in Germany evaluated treatment in a sample of 16 German preadolescents with Class III malocclusion to an untreated distant control group (from Univ. of Florence and Univ. of Michigan) of similar size, age, gender and malocclusion. For treatment, a hyrax RME appliance was fitted to molar bands and 2 mini-implants in the palate, so that both skeletal and dental anchorage was available. The appliance had buccal bars with hooks for elastic attachment to a face mask, and a force of ~400 grams was applied for 16 hours per day. The expansion device was activated 4 times a day with a quarter turn each time (expansion rate of 0.8 mm/day) until the maxillary arch was over-corrected for buccal overjet. Average treatment time was less than 6 months, but the end point was not specified. The results showed that the treatment group had mean 2.4 degree increase in ANB and 2.4 mm advancement of A point, while the control group had a mean 0.4 degree decrease in ANB and 0.4 mm backward movement in A point. Using the Mann-Whitney U test, the difference was statistically significant at the p <.05 level. In contrast to facemask studies with dental anchorage only, the mean forward movement of the maxillary dentition was quite small and not significantly different from the controls. In the mandible, SNB decreased by a mean 1.7 degrees with a mean 1.9 mm distal change at Pogonion, and a statistically significant closing of the Co-Go-Me angle was observed. WHAT THE PROFESSOR THINKS The RME protocol was aggressive and without rationale, and since advancement of the maxilla increases the width of the maxillary arch relative to the mandible, that could create crossbite problems later. But, these are good short-term changes in both the maxilla and mandible with a relatively noninvasive treatment method. The magnitude of skeletal change is in the realm of several other face mask techniques. The lack of dental compensation and vertical control were impressive. It will be important to see what the stability of the results are in long term follow-up, and to keep in mind the large variability in the outcomes within both groups—the mean changes reported here are not good predictors of the treatment outcome with individual patients. Article Reviewed: Nienkemper M, Wilmes B, Franchi L, Drescher D. Effectiveness of maxillary protraction using a hybrid hyrax-facemask combination: A controlled clinical study. Angle Orthod 85: 764-70, 2015 (Sept).
0 Comments
|
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed