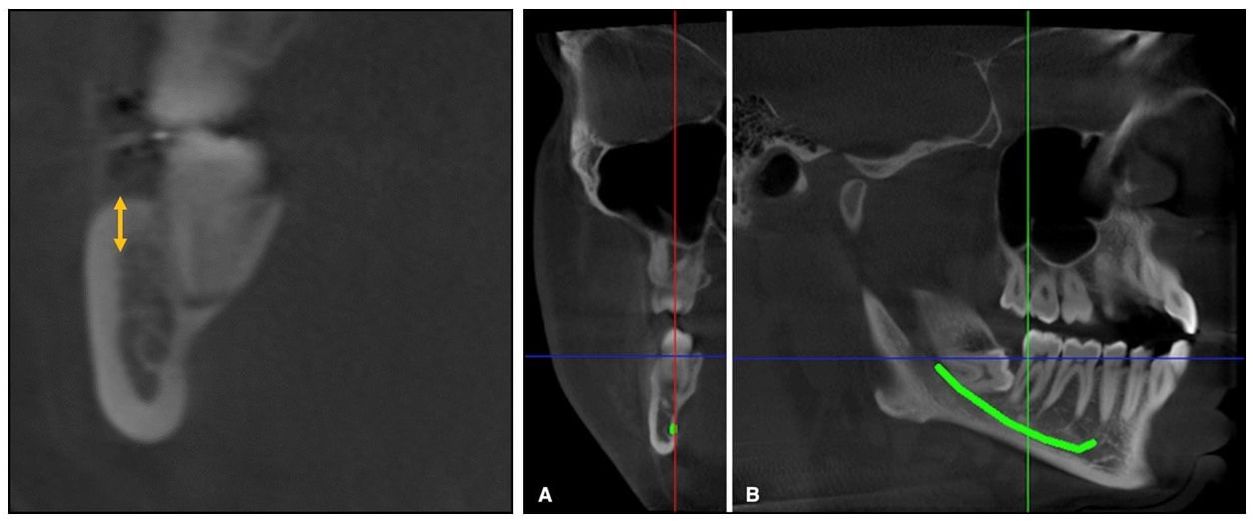
 From Elshebiny et al. Coronal slice at the distal of the second molar (left), and the traced inferior alveolar canal (A and B). From Elshebiny et al. Coronal slice at the distal of the second molar (left), and the traced inferior alveolar canal (A and B). By WILLIAM R. PROFFIT, DDS, PhD STUDY SYNOPSIS At the Case-Western Reserve Dept. of Orthodontics, cone-beam CT images were used to evaluate the shape and location of the mandibular buccal shelf below the molars in white (European descent) patients as possible sites for skeletal anchorage. The cortical bone at this location has been used by orthodontists working with Asian patients, and excellent success (93%) with bone screws there has been presented.(1) The objectives in this study were to:
Cone-beam CT images for 30 adolescent white patients who had CBCT’s as part of their diagnostic evaluation were used to obtain a detailed view of the mandible in the first and second molar region (Figures 1 and 2). Cortical shelf thickness and the width of the buccal shelf bone were measured at the distal of the first molar and at the mesial and distal of the second molar. Then, the position of the mandibular nerve at these locations was established and its distance from a visual screw placed vertically was measured. The data showed that cortical bone thickness was greatest below the disto-buccal cusp of the second molar (8.1 + 1.3 mm), and that although this also was the point of greatest proximity to the mandibular neurovascular bundle (5.5 + 1.6 mm), this amount of clearance would provide adequate safety. Based on these measures, the authors recommended a 10 mm anchorage screw with a 5 mm screw head extension in this location. Locations below the first molar, not the second molar, have been recommended for Asian patients. Whether this recommendation is related to a clinically significant difference in mandibular anatomy between the two racial groups is not known. WHAT THE PROFESSOR THINKS
Alveolar bone screws have proved to be acceptable as anchorage for minor tooth movement but disappointing as anchorage for major tooth movement. For example, two clinical trials of a Nance lingual arch vs. alveolar bone screws for maxillary incisor retraction found no advantage with the bone screws—the two anchorage types were equally ineffective. It has become clear that cortical bone of the palate does offer almost perfect anchorage for intrusion, retraction and protraction of maxillary dental segments or the whole maxillary dental arch(2), and palatal anchorage now is preferred. Is the cortical bone of the buccal shelf of the mandible equally superior to mandibular alveolar bone? The existing data from Asian patients certainly indicates that for them, it is. This report for white adolescents shows that:
Based on these points, it is reasonable to expect bone anchors in the buccal shelf to be more stable than bone screws in the mandibular alveolus. However, there are no studies yet with high-quality outcome data for white patients to be certain that this is correct. Should American clinicians now start using bone screws into the mandibular buccal shelf for white as well as Asian patients when movement of mandibular segments or the whole mandibular arch is needed? On balance, I would say yes. Article Reviewed: Elshebiny T, Palomo JM, Baumgartel S. Anatomic assessment of the mandibular buccal shelf for miniscrew insertion in white patients. Am J Orthod Dentofac Orthop 2018; 153:505-511 (Apr). References
1 Comment
|
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed