 More crowding was associated with less A-P incisor movement and less space opening. More crowding was associated with less A-P incisor movement and less space opening. BY TUNG T. NGUYEN
STUDY SYNOPSIS This study, published in the January 2016 issue of the AJODO, followed 43 Class I patients treated with 4 bicuspid extractions for 5 years during retention. The mean age of the subjects was 13.6 +/- 1.4 at the start of treatment and 16.1 +/- 2.0 at the end of treatment. All subjects had maxillary Hawley retainers and mandibular 3-3 fixed retainers. Crowding, spacing, intercanine distance, and incisor angulation, along with multiple dental measurements were made for initial, final, 1-year and 5-year retention records. 30% of the patients had at least one extraction space reopen, with the majority occurring within the first year of retention. Extraction space tended to reopen more in the maxilla (2.5 to 1 ratio) than the mandible and often times only in 1 quadrant. In addition, the reopened extraction space tended to close at the 5-year retention point. WHAT THE PROFESSOR THINKS The extraction debate continues to be a source of controversy in our profession. We make decisions between expansion and extraction based on our practice philosophy / training, esthetic preferences, the degree of crowding, and of course, stability. Proponents of extraction will cite the stability of tooth movement as a major advantage. However, it may be the magnitude of tooth movement that has more to do with stability – not simply whether one extracts or expands. The authors found that the larger degree of incisor retraction and smaller the initial crowding, the more likely premolar extraction space were to reopen; ie: the farther you move teeth, the more likely they are to return to their original anterior-posterior (A-P) position. It is interesting to note that when the initial crowding was at least 11.63mm, none of these subjects showed space opening. When the initial crowding was only 8.39mm, these subjects had 2.6mm of incisor retraction and tended to show space opening. Could 2-3mm of AP movement of the incisor be the threshold for relapse? Unfortunately, the sample size is too small to make that assumption. The authors should have reported the size of the extraction space opening. 0.25-0.5mm is often clinically insignificant, whereas 1-2mm of space opening is often a source for interdental food impaction. It is important to note that extraction spaces tended to decrease at the 5-year retention mark. Was that due to late mandibular growth? Bjork’s studies have already hinted at that point, but we need more data. The Bottom Line: Regardless of whether you extract or not, careful consideration of retention strategy is needed, especially when teeth are moved greater distances. That is true for both growing and non-growing patients. Article Reviewed:Garib D, Bressane L, Janson G, Gribel B. Stability of extraction space closure. Am J Orthod Dentofacial Orthop 2016;149:24-30.
2 Comments
 Naoumova et. al. 2015 Naoumova et. al. 2015 BY WILLIAM R. PROFFIT & TATE H. JACKSON
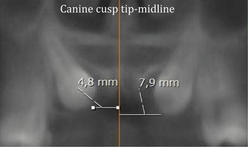
STUDY SYNOPSIS In a follow-up to Kurol’s classic studies, a prospective clinical trial was carried out in Gothenburg in which 67 patients age 10-13 with unilateral or bilateral palatally displaced permanent maxillary canines were randomly assigned to extraction or retention of maxillary primary canines. Clinical examination and CBCTs were obtained initially and at 6 and 12 months later; total observation time was 24 months. Significantly more spontaneous eruption of the permanent canines was seen in the extraction than control group (69% vs 39%), and faster eruption was noted in the extraction group. The relationship of the canine cusp tip to the midline was the best predictive measure of the outcome. If this distance was 11 mm or more, spontaneous eruption of the canine was achieved; if it was 6 mm or less, some positional improvement often occurred but surgical exposure was needed despite interceptive extraction of the primary canine. WHAT THE PROFESSOR THINKS It is important to note that the image analyses in this study were done using multi-planar views from 3D CBCT volumes. One advantage of using 3D images is that the distortion in observed canine position inherent to 2D images is avoided. For most clinicians who use 2D panoramic images everyday to assess canine position, the absolute numbers reported in this study must be used with some caution. Nonetheless, this study was well done and carries useful contemporary clinical guidelines. Specifically, early extraction of the primary canines is particularly indicated for patients with cusp tip to midline distances of 7-10 mm. When the distance from the cusp tip to the midline is less than 7mm, primary canine extraction can still be helpful in facilitating later surgical exposure. Article Reviewed: Naoumova J, Kurol J, Kjellberg H. Extraction of the deciduous canine as an interceptive treatment in children with palatally displaced canines--part I: Shall we extract the deciduous canine or not?; Part II: Possible predictors of success and cut-off points for a spontaneous eruption. Eur J Orthod 37: 209-218 and 219-229, 2015 |
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed