|
BY TATE H. JACKSON STUDY SYNOPSIS Newly published data from a group at Virginia Commonwealth University examines the accuracy of a smartphone app (in which patients scan their own teeth) in making linear dental measurements during rapid maxillary expansion. 12 patients (age 10-17 years, 4 males) for whom rapid maxillary expansion using a Hyrax appliance was planned were enrolled as a prospective cohort. At baseline, the patients were trained in the use of the app Dental Monitoring (Paris, France). Patients all used the same Apple iPhone 6 Plus and the lip/cheek retractors provided by the company for use with the app while capturing video scans of their own teeth. Before Hyrax delivery, at the time of Hyrax delivery, and then weekly during active expansion, each patient made a scan of their own teeth using the same smartphone at the clinic, in a private room away from the study personnel. For comparison, study personnel also scanned each patient’s teeth using the same app and phone at each visit. Alginate impressions were also made at each visit to serve as a gold standard measure, along with intraoral measurements. Only at baseline was an intraoral scan also obtained using an iTero intraoral scanner.  Both patients and study personnel captured video scans of the patient’s teeth using a smartphone app at baseline and during expansion with a Hyrax appliance. From Moylan et al. Intermolar and intercanine width measurements were made during the course of expansion using data obtained with the app and compared to measurements made on plaster models. Repeatability of measurements made on the plaster models was high (ICC=0.99). 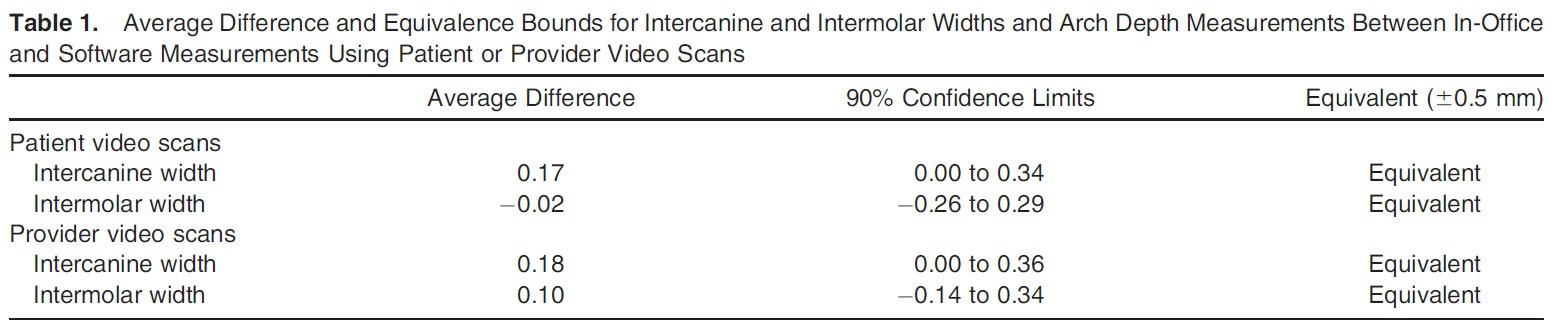 Table 1 Results from Moylan et al. In total, all intermolar and intercanine expansion measures calculated by the app were within 0.5mm of the measures made using plaster casts (Table 1 from Moylan et al). 3 of 58 video scans captured by the app (2 by patient and 1 by study personnel) were judged to be of poor enough quality to not be used for measurements.
WHAT THE PROFESSOR THINKS Although the sample size in the study was small, the fact that multiple video scans were obtained for each participant yielded enough data to draw interesting initial conclusions. The study was well-designed in that the two linear measurements that were evaluated have great clinical significance in the context of rapid maxillary expansion. Similarly, having all patients use the same phone in a private setting away from examiners was logical for the aim of the study, which was to determine the accuracy of patient-obtained intraoral scans using a smartphone. If patients had used a variety of phones in an uncontrolled setting, more confounding variables might have been introduced. This study is well-placed for the current state of orthodontic practice. If a smartphone app can deliver accurate information regarding tooth position that is clinically acceptable (and 0.5mm was a reasonable threshold in this study), certainly clinicians should be open to the judicious use of similar technology for the best care of our patients. In this case, monitoring Hyrax expansion remotely with fewer in-office visits, might be possible. These data do not suggest that “selfie-orthodontics” is appropriate. They do, however, provide good initial data to suggest that orthodontists might have the opportunity to ethically embrace such technology as another tool to provide optimal care. Article reviewed: Heather B. Moylan; Caroline K. Carrico; Steven J. Lindauer; Eser Tu¨ fekci¸. Accuracy of a smartphone-based orthodontic treatment–monitoring application: A pilot study. Angle Orthodontist. Online 2019.
1 Comment
|
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed