 TDI's (Traumatic Dental Injuries) have multiple risk factors - more than just OJ. TDI's (Traumatic Dental Injuries) have multiple risk factors - more than just OJ. BY LORNE D. KOROLUK
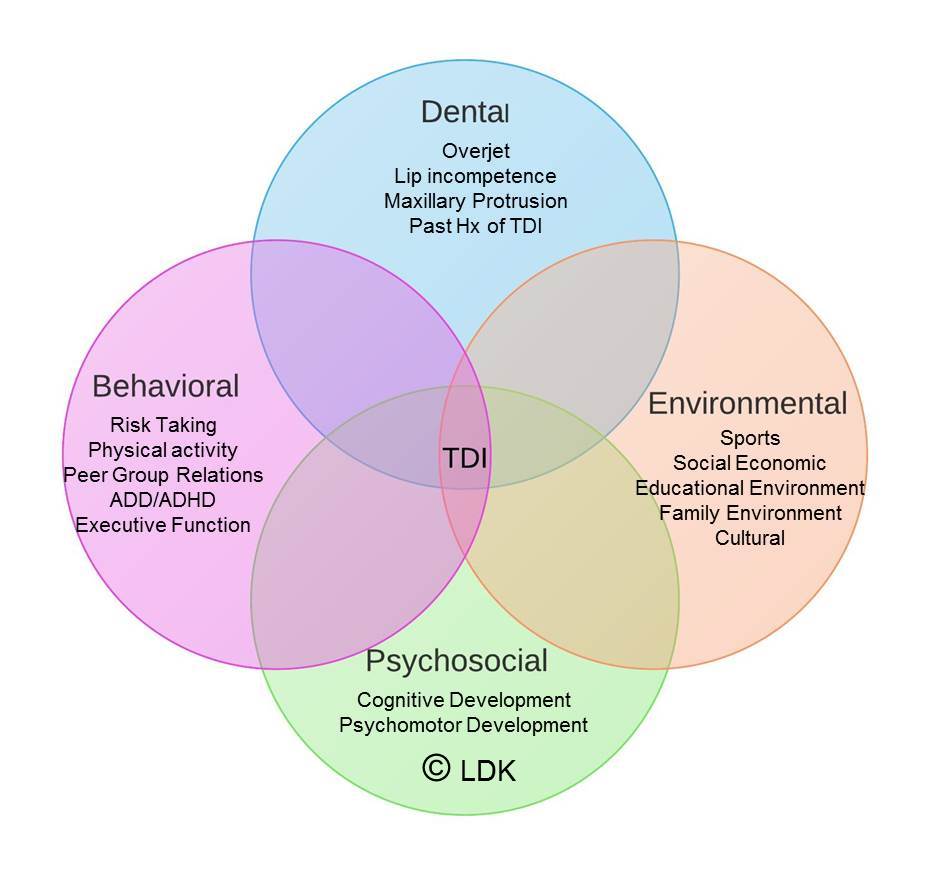
STUDY SYNOPSIS A recent study in the AJO-DO summarized findings from a Cochrane Review that re-investigated evidence regarding orthodontic treatment for prominent maxillary incisors and Class II malocclusion in children. The authors identified three randomized clinical trials (Florida, North Carolina, and United Kingdom) that compared outcomes of two-phase treatment in the mixed dentition and permanent dentition versus single phase treatment in the permanent dentition. Data from all three clinical trials showed no statistically significant difference between final overjet, final ANB, final PAR score and self-concept score. Early functional appliance therapy, however, was shown to reduce the risk of incisor trauma which was reported as a number needed to treat (NNT=10). This suggests an orthodontist must treat 10 such patients in order to prevent 1 incidence of new incisal trauma. Analysis of early headgear treatment in the North Carolina and Florida studies showed a significant reduction in the risk for new incisor trauma that prevented 1 incidence of new trauma for every 6 patients treated. No differences were found between early functional appliance and headgear treatment for all variables, including incidence of trauma. In the discussion the authors raise some very salient issues and advise caution interpreting the results. The authors conclude that there are no advantages in providing 2-phase treatment compared to single-phase treatment in early adolescence, except for a potential reduction in risk for new incisor trauma. WHAT THE PROFESSOR THINKS The authors have used systematic review and meta-analysis to combine data from three groups of randomized clinical trials to increase the power of the statistical analysis. In the analysis, trauma is very simplistically defined as new incisor trauma versus no new incisor trauma. Incisor trauma consists of a very wide continuum ranging from minor craze lines and enamel fractures to very serious fractures, luxations and avulsion. The Florida and North Carolina studies used the Ellis and NHANES III classifications respectively to identify the severity of new trauma. The United Kingdom study did not rate the severity of trauma, but instead simply coded trauma as yes or no. Readers must very carefully apply these findings to individual patients. The yes / no definition of new incisor trauma over-simplifies the clinical implications of the findings. Further, there was wide variability associated with the NNT statistics reported. Careful scrutiny of the statistical analysis shows that risk reduction with the functional appliance could range from 2% to 54% and from 13% to 61% for headgear. Similarly, the confidence intervals for the measure of treatment impact as NNT are quite large: 5 to 175 for functional appliance and 3 to 23 for headgear. The most important sentence in this article is, “the prevention of trauma should not be the only reason for routinely providing treatment for Class II malocclusion. The decision should be taken as part of a risk evaluation….” The existing literature, without question, has shown that increased overjet is a significant risk factor for traumatic dental injuries and incisor trauma. Logically, one can infer that reducing overjet should reduce future trauma. Overjet, however, is not the sole risk factor. Dental factors such as overjet, lip incompetence, maxillary protrusion, Class II relationship, and past history of dental trauma are important risk factors. Psychosocial, environmental, and behavioral factors also determine an individual’s future risk. Behavioral and psychosocial factors may be even more important that dental factors, since they place the individual and their teeth in the at-risk situations in the first place. Clinicians must compare the cost of potentially lengthy orthodontic treatment to reduce risk of incisor trauma to the cost of treating incisor trauma and its potential future sequelae. One of the North Carolina studies(1) showed that the expected-cost of new incisor trauma was significantly less than the cost of orthodontic intervention to reduce future risk. Hopefully clinicians (and organized orthodontics) don’t ignore the numerous cautionary warnings by the authors. A narrow interpretation of the results to justify early orthodontic treatment as a necessity for all children in the mixed dentition with increased overjet is certainly not an evidence-based conclusion. Article Reviewed: Thiruvenkatachari B, Harrison J, Worthington H, O'Brien K. Early orthodontic treatment for Class II malocclusion reduces the chance of incisal trauma: Results of a Cochrane systematic review. Am J Orthod Dentofacial Orthop 2015;148:47-59 References:
1 Comment
|
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed