 Advancing the mandible further does not necessarily lead to a lower AHI. Advancing the mandible further does not necessarily lead to a lower AHI. BY TATE H. JACKSON
STUDY SYNOPSIS An Italian group has published a systematic review and meta-analysis that holds some practical clinical information for orthodontists or dentists using mandibular repositioning appliances to treat obstructive sleep apnea. The authors followed PRISMA guidelines and reviewed publications from 1990 – 2015. Only randomized controlled trials were included in the analysis of the association between reduction in apnea-hypopnea index (AHI) and therapy with a mandibular repositioning device in adults. Importantly, all changes in sleep-disordered breathing were measured by polysomnography (PSG) – both at baseline and after treatment. 13 studies were included in the analysis. Successful reduction in AHI (reduction of sleep apnea) was found in studies where the mandible was advanced as little as 25% of the maximum protrusion possible. Advancement of 50% showed equivalent results to advancements of a greater magnitude. Although the treatment modality was effective in significantly reducing AHI, no clear association between advancing the mandible further and a greater reduction in AHI could be made. Since variability in individual response was reported, the authors suggested a conservative and personalized approach to treatment by initially posturing the mandible forward only “the minimum effective” distance. WHAT THE PROFESSOR THINKS Although the authors conclude that the 13 RCT’s included in this meta-analysis represent a relatively small body of evidence of moderate quality, the data presented have some strengths. Only randomized controlled trials where the outcome of interest was clearly defined were included. The “gold standard” of polysomnography was used to assess changes in sleep apnea in each study. Further, only studies that accounted for changes in BMI and considered patients over 18 were included. From an orthodontic perspective, posturing the mandible forward in a non-growing adult with a fixed or removable appliance could certainly have ramifications, both for the patient’s occlusion / alignment and for the patient's comfort / ability to tolerate the appliance. If protruding the mandible 50% of the maximum possible works, then tooth-movement side effects, as well as pain and discomfort, might be limited. Not posturing the mandible forward fully at baseline might also allow for future increases over time as needed. This article provides two key pieces of information for the clinician treating sleep apnea in adults with appliances that protrude the mandible:
As the enthusiasm for treating sleep apnea with mandible-posturing oral devices continues, these data may become more and more relevant for orthodontists – either as we provide treatment for sleep apnea, or as we address the potential changes in occlusion and alignment caused by such treatment. Article Reviewed: Bartolucci, et. al. The effectiveness of different mandibular advancement amounts in OSA patients: a systematic review and meta-regression analysis. Sleep Breath. Jan 2016
0 Comments
 Piezocision resulted in 7 months less treatment time, but 50% of the participants had gingival scarring. Piezocision resulted in 7 months less treatment time, but 50% of the participants had gingival scarring. BY TATE H. JACKSON
STUDY SYNOPSIS A group from Belgium has published results of a Randomized Controlled Trial to evaluate the effect of flapless corticotomies on tooth movement. 24 consecutively-treated adult patients were randomized to 2 groups: 1) a control group treated with non-extraction alignment or 2) an intervention group treated with non-extraction alignment and piezocision one week after brackets were bonded. All participants had similar malocclusions with only mild – moderate crowding. Both groups were treated using self-ligating brackets (Damon) and a standardized archwire sequence with a 2 week recall interval. A single blinded orthodontist validated readiness for appliance removal – or gave guidance for further adjustments to be made – based on an evaluation of dental casts and “5 criteria”. For the intervention group, piezocision was accomplished using a 5mm x 3mm piezoelectric device apical to each interdental papilla. An incision was created before the corticotomy, but no sutures were used. Where root proximity might be a concern, corticotomy was avoided. For the piezocision group, treatment was 43% faster. That means that the total treatment time was about 7 months less (about 11 months of total treatment time vs. 18 months in the control group). As treatment proceeded, the difference decreased between the two groups in terms of time spent in each archwire, suggesting a decreasing effect of the corticotomies over time. No adverse outcomes in terms of periodontal health or root resorption were reported – nor were there any apparent differences (increase or decreases) in alveolar bone support or thickness, as assessed by CBCT. 50% of patients experienced some degree of scarring. WHAT THE PROFESSOR THINKS Despite some minor drawbacks, this study is one that provides some useful information to clinicians with a patient population who demand accelerated treatment. A description of the randomization process and the “5 criteria” used to determine if treatment was complete would be very helpful. Nonetheless, using a single blinded examiner who evaluated casts and used objective criteria to determine when treatment was complete for both the piezocision and the control groups was a clever design. Using total treatment time as the outcome, rather than just the time to initial alignment, makes the study results more relevant to practicing clinicians. As in previous reports, the acceleratory phenomenon was limited to a period of time early in treatment (the authors suggest about 4 months). For non-extraction patients with mild-moderate crowding, a single procedure was enough to yield a clinically-relevant reduction in treatment time of 7 months. It is imperative to note that the reported recall rate during treatment was 2 weeks. That means treatment is accelerated, but it is no more efficient for the patient or the orthodontist – since an increased number of office visits would be required. The findings presented in this study suggest that less-invasive piezocision may carry with it a low risk of adverse outcomes. No participants experienced a loss of root structure or bony support, as judged using CBCT. Interestingly however, half of the piezocision participants did experience scarring of the gingiva, an outcome that could have very negative effects on a patient with a high esthetic demand. For the practicing orthodontist, this study carries with it some helpful information to guide patients when they ask for quicker treatment: Will treatment time be shorter? Yes. By how much? About 7 months. Are there risks? Yes – and we still do not know the full extent of those risks, including the esthetic risk of scarred gingiva. Will it be more convenient? No. (Remember, the reported recall interval in this study was 2 weeks.) Article Reviewed: Charavet C, et al. Localized Piezoelectric Alveolar Decortication for Orthodontic Treatment in Adults: A Randomized Controlled Trial. J Dent Res. April 2016. 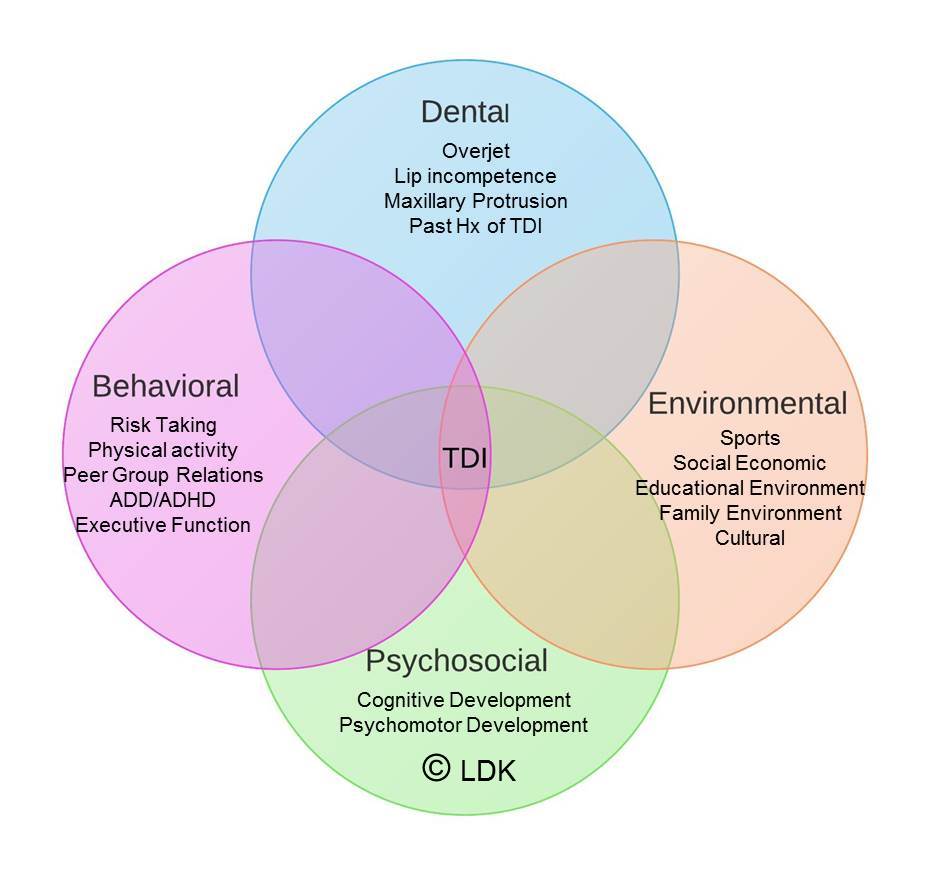 TDI's (Traumatic Dental Injuries) have multiple risk factors - more than just OJ. TDI's (Traumatic Dental Injuries) have multiple risk factors - more than just OJ. BY LORNE D. KOROLUK
STUDY SYNOPSIS A recent study in the AJO-DO summarized findings from a Cochrane Review that re-investigated evidence regarding orthodontic treatment for prominent maxillary incisors and Class II malocclusion in children. The authors identified three randomized clinical trials (Florida, North Carolina, and United Kingdom) that compared outcomes of two-phase treatment in the mixed dentition and permanent dentition versus single phase treatment in the permanent dentition. Data from all three clinical trials showed no statistically significant difference between final overjet, final ANB, final PAR score and self-concept score. Early functional appliance therapy, however, was shown to reduce the risk of incisor trauma which was reported as a number needed to treat (NNT=10). This suggests an orthodontist must treat 10 such patients in order to prevent 1 incidence of new incisal trauma. Analysis of early headgear treatment in the North Carolina and Florida studies showed a significant reduction in the risk for new incisor trauma that prevented 1 incidence of new trauma for every 6 patients treated. No differences were found between early functional appliance and headgear treatment for all variables, including incidence of trauma. In the discussion the authors raise some very salient issues and advise caution interpreting the results. The authors conclude that there are no advantages in providing 2-phase treatment compared to single-phase treatment in early adolescence, except for a potential reduction in risk for new incisor trauma. WHAT THE PROFESSOR THINKS The authors have used systematic review and meta-analysis to combine data from three groups of randomized clinical trials to increase the power of the statistical analysis. In the analysis, trauma is very simplistically defined as new incisor trauma versus no new incisor trauma. Incisor trauma consists of a very wide continuum ranging from minor craze lines and enamel fractures to very serious fractures, luxations and avulsion. The Florida and North Carolina studies used the Ellis and NHANES III classifications respectively to identify the severity of new trauma. The United Kingdom study did not rate the severity of trauma, but instead simply coded trauma as yes or no. Readers must very carefully apply these findings to individual patients. The yes / no definition of new incisor trauma over-simplifies the clinical implications of the findings. Further, there was wide variability associated with the NNT statistics reported. Careful scrutiny of the statistical analysis shows that risk reduction with the functional appliance could range from 2% to 54% and from 13% to 61% for headgear. Similarly, the confidence intervals for the measure of treatment impact as NNT are quite large: 5 to 175 for functional appliance and 3 to 23 for headgear. The most important sentence in this article is, “the prevention of trauma should not be the only reason for routinely providing treatment for Class II malocclusion. The decision should be taken as part of a risk evaluation….” The existing literature, without question, has shown that increased overjet is a significant risk factor for traumatic dental injuries and incisor trauma. Logically, one can infer that reducing overjet should reduce future trauma. Overjet, however, is not the sole risk factor. Dental factors such as overjet, lip incompetence, maxillary protrusion, Class II relationship, and past history of dental trauma are important risk factors. Psychosocial, environmental, and behavioral factors also determine an individual’s future risk. Behavioral and psychosocial factors may be even more important that dental factors, since they place the individual and their teeth in the at-risk situations in the first place. Clinicians must compare the cost of potentially lengthy orthodontic treatment to reduce risk of incisor trauma to the cost of treating incisor trauma and its potential future sequelae. One of the North Carolina studies(1) showed that the expected-cost of new incisor trauma was significantly less than the cost of orthodontic intervention to reduce future risk. Hopefully clinicians (and organized orthodontics) don’t ignore the numerous cautionary warnings by the authors. A narrow interpretation of the results to justify early orthodontic treatment as a necessity for all children in the mixed dentition with increased overjet is certainly not an evidence-based conclusion. Article Reviewed: Thiruvenkatachari B, Harrison J, Worthington H, O'Brien K. Early orthodontic treatment for Class II malocclusion reduces the chance of incisal trauma: Results of a Cochrane systematic review. Am J Orthod Dentofacial Orthop 2015;148:47-59 References:  If treatment begins during the mixed dentition, a longer transitional dentition phase may lead to longer treatment time. If treatment begins during the mixed dentition, a longer transitional dentition phase may lead to longer treatment time. BY TATE H. JACKSON
STUDY SYNOPSIS A recent study published in the Angle Orthodontist compared two cohorts of children in Finland in terms of the timing of eruption of permanent teeth. The historic group of children born from 1976-1980 included more than 1,500 children from rural parts of the country. The more recent group, born from 1999-2002, included 483 children who lived in a less rural environment and were followed longitudinally. Permanent tooth eruption was observed clinically and graded using consistent criteria for both groups. Two age ranges were the focus of the study: 1) age 6-9 years, to include the early mixed-dentition transition and 2) age 9-12 years, to include the late transition to permanent dentition. Compared to the 1980 group, the 2000 group showed more advanced permanent tooth eruption during the first age range (6-9 years). There was no difference, however, in permanent tooth eruption between the 1980 and 2000 groups when considering the second age range (9-12 years). So, although teeth began to erupt earlier in the 2000 group, the full transition to permanent dentition was completed no quicker than the group observed 20 years earlier. Effectively, the 2000 group had a longer transitional phase from primary to permanent dentition. WHAT THE PROFESSOR THINKS The authors compared cross-sectional observations of eruption stage for a historic group to a modern group who were followed longitudinally. To help account for one of the evident drawbacks of this design, the statistical analysis appropriately accounted for differences in age distribution between the groups. Further, few studies include any good longitudinal data of this sort. This report of a secular trend – that the emergence of permanent teeth is occurring at an earlier age compared to many years ago – is worth consideration by clinicians. Especially since this finding means that the transitional dentition phase is effectively longer. Put in a clinical context, this study implies that the orthodontist who begins comprehensive treatment for children in the mixed dentition because they appear to be advanced dentally may find that they also have longer treatment times. Why? Because all of the permanent teeth did not finish erupting on the apparently accelerated pace that was initially observed. It is unfortunate that the magnitude of the secular trend effect was not reported in a meaningful way in this study. So how should clinicians use these data? These data find utility when combined with individual clinical experience. For the orthodontist who suspects that he or she is waiting on the eruption of permanent teeth longer today than a few years ago, this study provides some evidence to trust their clinical judgement – and not rush to start patients younger and thereby sacrifice treatment efficiency. Article Reviewed: Eskeli, Losonen et al. Secular trends affect timing of emergence of permanent teeth. Angle Orthod. 86:53-58. 2016 (Jan.)  Lombardo et al. 2015 Lombardo et al. 2015 BY HENRY W. FIELDS
STUDY SYNOPSIS Several factors affect the expression of the third order (torque) configuration of archwires upon teeth. These include the bracket slot size, wire dimension, and the bevel of the edge of square and rectangular wires. These variables have been examined in the past, but this recent study combined all three aspects for 43 archwires of different wire sizes and types using a digital gauge and micrographs measured with digital image software. The wires came from six manufacturers. Each wire was examined using 3 samples. The results demonstrated that there is substantial variation within each wire for each manufacturer. Wire width and height were both under and over-sized—many significantly so. Some manufacturers displayed sizing tendencies, but all had significant differences from the ideal nominal sizes. Corner radiuses were present (not 90 degrees) in all of the samples, and often there were four different radii for one wire (each corner was a different shape). The wire material affected sizing as well. Coated wires were the most true to size, followed by NiTi and TMA. Steel and tempered steel were the most undersized. WHAT THE PROFESSOR THINKS These results, along with the knowledge that most bracket slots are oversized, leads to more problems than expected in expressing torque in tooth movement. The undersized wires and corner bevels lead to a considerable amount of play (rotation before expressing a moment) between the bracket and rectangular wire. This difference can be considerably larger than ideal and up to 3 times what is expected. Unfortunately, since the cross-sectional size and shape of commercially-available wires are highly variable, straightwire clinicians are likely to encounter difficulty in torquing unexpectedly. . . and more frequently than desired. For the clinician who wants more ideal torque, the options are 1) to increase the wire size, which is perhaps a better option when using TMA wires so that harsh forces are not produced 2) purchase high torque brackets for potential problem cases or 3) consider torquing auxiliaries or archwire bends. Article Reviewed: Lombardo L, Arreghini A, Bratti E et al. Comparative analysis of real and ideal wire-slot play in square and rectangular archwires. Angle Orthod 85: 848-58, 2015 (Sept). |
Curated by:
Tate H. Jackson, DDS, MS CategoriesArchives
October 2019
|
 RSS Feed
RSS Feed